Next-gen weight-loss drugs at ADA 2026 — Phase 3 highlights

ADA 2026 Recap: What the Biggest Diabetes Meeting of the Year Means for Your Health
The ADA's 86th Scientific Sessions in New Orleans produced landmark shifts in diabetes care: heart and kidney protection is now a co-equal goal alongside blood sugar control, CGMs are proven to help non-insulin type 2 patients, a 29% heart event reduction from Repatha in high-risk diabetics, and four next-generation weight-loss drugs with remarkable Phase 3 data. Plus cardiovascular and liver disease updates.
The most talked-about week on the diabetes calendar just wrapped up. From June 5 to 8, the American Diabetes Association (ADA) held its 86th Scientific Sessions in New Orleans, and the news coming out of it touched every person managing diabetes, heart disease, or metabolic liver disease. A landmark study proved that continuous glucose monitors (CGMs) help type 2 patients who don't use insulin. New guidelines officially moved heart and kidney protection up to the same level as blood sugar control. And a remarkable lineup of next-generation weight-loss drugs showed clinical trial data that researchers described — carefully, and with important caveats — as unlike anything seen before. Here's what it all means for you this week.
Diabetes: the ADA meeting rewrites several ground rules
Protecting your heart and kidneys is now a co-equal goal of diabetes care
The most significant shift in this year's ADA Standards of Care — the clinical guidelines your doctor follows for managing diabetes — is a change in priorities. 1 For years, lowering blood sugar (A1c) was the primary target, and protecting the heart and kidneys came second. The 2026 standards change that: cardiovascular and kidney risk reduction is now a co-primary goal, on equal footing with blood sugar control.
What this means in practice:
- Two drug classes — GLP-1 receptor agonists (like semaglutide/Ozempic and tirzepatide/Mounjaro) and SGLT2 inhibitors (like empagliflozin/Jardiance and dapagliflozin/Farxiga) — are now recommended as core heart and kidney protection for patients who have cardiovascular or kidney disease, regardless of whether their A1c is already at goal. The point is no longer "use these only if blood sugar isn't controlled"; it's "use these to protect your heart and kidneys even if your A1c looks fine."
- The blood pressure target has been updated: the guidelines now encourage reaching a systolic blood pressure (the top number) below 120 mmHg in patients who can safely achieve it, compared to the previous target of below 130 mmHg.
- CGMs are now the recommended blood sugar monitoring method for all ages — including children and adolescents — with both type 1 and type 2 diabetes.
- A medication called finerenone (brand name Kerendia) — a non-steroidal mineralocorticoid receptor antagonist (MRA), meaning it works on a specific hormone pathway in the kidneys and heart — received formal recognition in the guidelines for reducing heart failure risk in people with diabetes and chronic kidney disease.
Dave Dixon, PharmD (Virginia Commonwealth University, expert contributor to the cardiovascular chapter of the 2026 ADA Standards), put it plainly: "The most meaningful evolution is that cardiovascular and kidney risk reduction is no longer treated as secondary to glucose lowering." 1
What to discuss at your next appointment: Ask your doctor whether your current medication plan addresses both blood sugar and heart/kidney protection — and whether a GLP-1 receptor agonist, SGLT2 inhibitor, or finerenone belongs in your regimen based on your individual risk profile.
A randomized trial confirms: CGMs help type 2 patients who don't use insulin
For a long time, continuous glucose monitors were considered standard equipment for type 1 diabetes and for type 2 patients on insulin — but there was little solid evidence that they mattered for the much larger group of type 2 patients managing with oral medications or non-insulin injectables. The CONNECT trial, presented June 6 at ADA 2026, fills that gap directly. 2
The trial enrolled 283 adults with type 2 diabetes (not on insulin) across 22 primary care clinics in the US. Half used a Dexcom G7 CGM; half received usual care. After 26 weeks:
- The CGM group reduced their A1c by 0.9 percentage points more than the usual-care group — a meaningful difference on top of the roughly 1.6% average reduction both groups saw.
- The CGM group spent 5 more hours per day with blood sugar in the target range (70–180 mg/dL).
- 82% of CGM users improved their blood glucose levels; CGM users also reported higher satisfaction with their monitoring and lower diabetes-related distress.
The average age was 60, about a third of participants were from racial or ethnic minority groups, and 37% were already on SGLT2 inhibitors, so this isn't a highly selected academic population — it looks like the real primary care world.
Thomas Martens, MD (study co-author), noted that "since many of the patients with type 2 diabetes who use oral or non-insulin injectable therapies are seen in primary care settings, continuous glucose monitoring provides an opportunity to close a visible care gap." 2
What to discuss: If you have type 2 diabetes and are not on insulin, ask your primary care doctor whether a CGM makes sense for you — and whether it would be covered by your insurance plan.
Repatha cuts heart attacks and strokes by 29% in high-risk diabetes patients
For people with diabetes who are at elevated heart risk but haven't had a heart attack or stroke yet, new data presented at ADA 2026 strengthens the case for aggressive cholesterol management. Amgen's evolocumab (brand name Repatha) — a PCSK9 inhibitor, meaning it blocks a protein that would otherwise prevent the liver from clearing LDL ("bad") cholesterol — reduced the first major heart event (combined risk of heart disease death, heart attack, or stroke) by 29% in a high-risk diabetes subgroup of 6,002 patients. 3
The patients in this subgroup had diabetes with at least one of the following: signs of small blood vessel damage (called microvascular complications), current insulin use, or diabetes duration of 10 or more years — and crucially, none had previously had a heart attack or stroke. Repatha was added on top of statin therapy, and the median LDL level in the Repatha group dropped to 45 mg/dL, compared to 106 mg/dL in the placebo group. Results were published simultaneously in Diabetes Care. 3
What to discuss: If you have diabetes with any of the risk features above and your LDL remains above 70 mg/dL on statin therapy, ask your cardiologist or endocrinologist whether a PCSK9 inhibitor belongs in your regimen.
A new generation of weight-loss drugs: four candidates at ADA 2026
The bulk of ADA 2026 conversation centered on a wave of next-generation obesity and diabetes drugs in late-stage development. None are approved yet — what follows is a summary of where each stands, to help you follow this story as it develops.
| Drug | Company | How it works | Key data presented at ADA 2026 | Development stage |
|---|---|---|---|---|
| Retatrutide | Eli Lilly | Weekly injection; activates three hormone receptors (GIP, GLP-1, and glucagon — called a "triple agonist") | TRIUMPH-1 (obesity, N=2,339): 28.3% weight loss (avg. ~70 lbs) at 80 weeks; 65% of participants dropped out of the obese BMI range. TRANSCEND-T2D-1 (type 2 diabetes, N=537): 2.0% A1c reduction, 46% reached normal blood sugar. Published in The Lancet. 4 | Phase 3 (trials ongoing); FDA submission not yet announced |
| CagriSema | Novo Nordisk | Weekly injection; combines two hormones — cagrilintide (amylin analogue) + semaglutide 2.4 mg | REIMAGINE 2 (T2D on metformin, N=2,713): A1c reduced 1.91%, weight reduced 14.2% — both superior to semaglutide alone. NDA for obesity already filed (Dec 2025), FDA decision expected Q4 2026. Published in The Lancet and The Lancet Diabetes & Endocrinology. 5 | Phase 3 complete; FDA review underway for obesity |
| Aleniglipron | Structure Therapeutics | Once-daily oral pill; small-molecule GLP-1 receptor agonist | Phase 2b (ACCESS): up to 16.2% weight loss in extended follow-up. Published in Nature Medicine. Phase 3 planned for Q3 2026. 6 | Phase 2b complete; Phase 3 starting Q3 2026 |
| Berobenatide | Pfizer | Once-monthly injection; extra-long-acting GLP-1 receptor agonist | Phase 2b VESPER-3: 12.3% weight loss at 28 weeks; T2D trial showed 2.2% A1c reduction. Phase 3 VESPER-6 now recruiting. 7 | Phase 2b complete; Phase 3 recruiting |
Loading stats card…
A few important context points for patients reading this table:
All four drugs remain investigational — none are approved for use outside clinical trials. Retatrutide and CagriSema produced the largest weight loss numbers seen in obesity drug trials, but independent researchers raised valid questions about tolerability (nausea affected up to 42% of retatrutide users) and some safety signals (rare heart rhythm irregularities in the smaller T2D retatrutide study) that need follow-up in larger trials. 4 8 Alice Y.Y. Cheng, MD (University of Toronto, independent commentator), asked a question worth holding: "Is bigger always better? Is bigger always needed? And is bigger always right? And the answers are no, no, and no." 8
If you are currently taking semaglutide, tirzepatide, or another approved GLP-1 medication, your treatment is not changing. These new drugs are in trials, not pharmacies. Watching which ones receive FDA submissions in the next 12–18 months will be the meaningful signal.
Cardiovascular: GLP-1 drugs, heart transplants, and an LDL gap
GLP-1 medications linked to 44% lower mortality in people with obesity and autoimmune disease
A study published June 6 in the Journal of the American Heart Association found that among 26,408 adults with both obesity and at least one autoimmune condition, those who used GLP-1 receptor agonist medications had a 44% lower risk of dying from any cause, a 31% lower risk of pulmonary embolism (blood clot in the lungs), and a 17% lower risk of venous thromboembolism (blood clots overall), compared to those who didn't use GLP-1 drugs. 9
The study used real-world electronic health records from 14 health systems across Florida, Georgia, and Alabama (2014–2024). This is an observational study — it cannot prove the GLP-1 drugs caused the lower mortality, because healthier patients may be more likely to receive the drugs. But it is the first study designed specifically to examine GLP-1 effects in the high-risk group of people who have both obesity and autoimmune disease (conditions like rheumatoid arthritis, lupus, inflammatory bowel disease, and psoriasis). The finding was simultaneously presented at ADA 2026.
Amy Sheer, MD, MPH (University of Florida, study author), noted: "In this real-world analysis, we found a consistent signal toward fewer serious complications including blood clots and lower mortality among patients treated with GLP-1RA." 9 Fatima Cody Stanford, MD (Massachusetts General Hospital / Harvard Medical School, not involved in the study), called the 44% mortality reduction "a striking finding that demands our attention." 9
What to discuss: If you have an autoimmune condition along with obesity or diabetes, and you are not currently on a GLP-1 medication, ask your rheumatologist or primary care doctor whether one might be appropriate given this emerging evidence.
AHA launches a research network specifically for heart transplant patients
On June 3, the AHA announced its first-ever heart transplant research network — $4.5 million in funding distributed across 14 research centers and one coordinating center (led by Icahn School of Medicine at Mount Sinai), with four-year grants beginning July 1, 2026. 10
Why this matters to patients: about 4,500 heart transplants are performed in the US each year (a record), but more than 3,700 patients remained on the waiting list in 2025. Rejection detection is still largely done through invasive biopsies, immunosuppression medications have barely changed in 20 years, and Black patients and children face worse post-transplant outcomes. The network's three research priorities are earlier non-invasive rejection detection, safer immunosuppression, and a quality-improvement framework to reduce outcome disparities.
This is a funding and infrastructure announcement, not a new treatment — outcomes from this work are years away. It signals that the AHA sees heart transplant care as an area of serious unmet need.
Only 1 in 4 heart attack survivors is meeting LDL targets — a new trial aims to fix that
A study protocol published June 3 in Frontiers in Cardiovascular Medicine quantified a stubborn problem: despite clear guidelines recommending LDL ("bad" cholesterol) below 55 mg/dL in patients who have had a heart attack, registry data show that only 20–25% of post-heart attack patients actually achieve that target in real-world practice; in Germany, the rate is below 15%. 11
The HACOL-ACS trial (based at Hannover Medical School, Germany) is testing whether starting three oral cholesterol-lowering drugs back-to-back early after a heart attack can close that gap. Stage 1 uses a high-dose statin plus ezetimibe (a cholesterol absorption blocker); patients who haven't hit the 55 mg/dL target after six weeks move to Stage 2, adding bempedoic acid (an oral drug that reduces cholesterol production in the liver). Recruitment ran through early 2026; results are pending.
The gap this trial is addressing affects patients in the US as well. If you or a family member has had a heart attack or was recently treated for acute coronary syndrome, it is worth asking at your next cardiology appointment: "What is my current LDL level, what is my target, and are there medication adjustments that could help me get there?"
Liver disease: fatty liver's growing footprint, betaine, and a semaglutide eligibility update
How bad is the global fatty liver problem? 1.3 billion people, and growing
A major analysis published in The Lancet using Global Burden of Disease 2023 data estimated that 1.3 billion people worldwide — about 16% of the global population — had metabolic dysfunction-associated steatotic liver disease (MASLD, commonly called fatty liver disease) in 2023. 12 That is a 143% increase in the total number of cases since 1990. The study projects the number will reach 1.8 billion by 2050, driven largely by population growth in sub-Saharan Africa and the Middle East/North Africa.
In the US context, MASLD affects an estimated 55% of people with type 2 diabetes and up to 64% of people with obesity. The leading risk factors, ranked by disease burden contribution, are high fasting blood sugar, high BMI, and smoking — the same constellation that drives diabetes and cardiovascular disease. This overlap is why doctors increasingly refer to these conditions together rather than treating each one in a separate specialty.
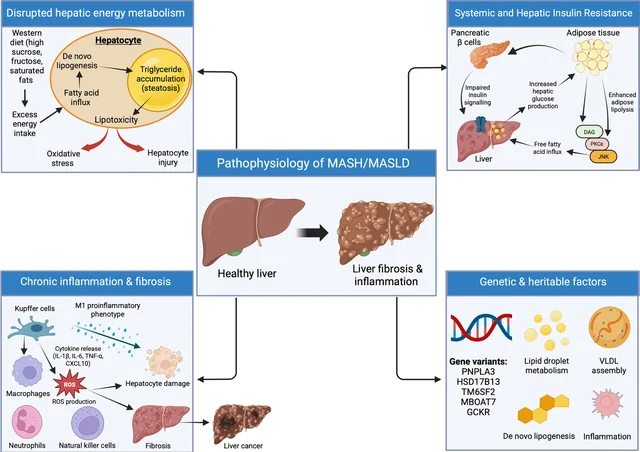
The figure below shows how MASLD progresses from fatty liver (steatosis) to inflammation (MASH — metabolic-associated steatohepatitis), scarring (fibrosis), and eventually cirrhosis or liver cancer if untreated.
Betaine (a supplement-like compound) shows liver benefit in MASLD pilot trials
Three pilot trials published in the June 2026 issue of Hepatology — the flagship journal of the American Association for the Study of Liver Diseases (AASLD) — tested oral betaine in adults with clinically confirmed MASLD who had elevated liver enzymes (ALT at or above 50 U/L). 14
Betaine (trimethylglycine) is a naturally occurring compound found in beets, spinach, and whole grains, and is also available as a dietary supplement. The three trials tested different doses and durations:
- 8 g/day and 4 g/day for 12 weeks (Trial 1, n=44): significant reductions in ALT, AST, cytokeratin-18 (a marker of liver cell death), and pro-C3 (a marker of liver scarring), compared to baseline. HDL ("good") cholesterol increased. LDL was unchanged.
- 2 g/day for 24 weeks (Trial 3, n=16): similar significant improvements.
- 1 g/day for 24 weeks (Trial 2, n=10): no significant changes observed — suggesting a minimum effective dose above 1 g/day.
About 35% of participants reported mild, short-lived gastrointestinal symptoms (nausea, loose stools) that resolved on their own.
A few important qualifications: these are small pilot studies, not the large phase 3 trials that establish a treatment as standard of care. Betaine is available over the counter as a supplement in the US, but supplements are not regulated the same way as prescription drugs — purity, dose accuracy, and quality vary by brand. Do not start taking betaine for your liver based on these pilot results without talking to your hepatologist or gastroenterologist first.
What to discuss: If you have MASLD with elevated liver enzymes and want to know whether betaine could play a role in your management, bring this paper to your next appointment with a specific question: "Are the doses studied here safe and reasonable to consider alongside my current treatment?"
If you have fatty liver disease, you almost certainly already qualify for semaglutide — the new liver indication adds very few people
Semaglutide (Ozempic/Wegovy) received FDA approval in 2024 for treating fibrotic MASH (metabolic-associated steatohepatitis with liver scarring), in addition to its existing approvals for type 2 diabetes and obesity. You might assume that new liver indication opened the door for a large group of patients who couldn't access semaglutide before. A study published June 4 in Gastro Hep Advances, reported by AGA's GI & Hepatology News, suggests the opposite is true. 15
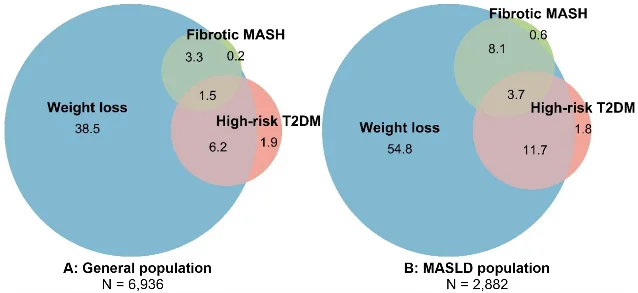
Researchers analyzed NHANES 2017–2020 data for 6,936 US adults and a validation group of 213 German patients with biopsy-confirmed MASLD. Their findings:
- In the general US adult population, 52% already qualified for semaglutide through its obesity or high-risk diabetes approvals. Adding the new MASH indication raised that percentage by less than one percentage point (from 51.8% to 51.8–52.0%).
- Among people already diagnosed with MASLD, 81% already qualified based on obesity or diabetes alone.
- Among those with the most serious liver disease (fibrotic MASH), 95% already qualified for semaglutide through a non-liver indication. Only 5% would be "new" candidates solely because of the liver approval.
Mohamed Elsaid, PhD, MPH (Ohio State University), summarized the real implication: "In metabolic liver disease, the obesity patient, the diabetes patient, and the liver patient are usually one person." 15 The larger problem isn't eligibility — it's that many of these patients are being managed in separate clinics (endocrinology, primary care, gastroenterology) without anyone connecting the dots to start them on the treatment.
Zobair Younossi, MD, MPH (Global NASH/MASH Council chair), added that "although candidacy for GLP-1 receptor agonists is high, penetration of use for MASH treatment remains suboptimal." 15
What to discuss: If you have been diagnosed with fatty liver disease and also have obesity or type 2 diabetes but are not currently taking a GLP-1 medication, ask the doctor managing your liver condition whether a GLP-1 is appropriate — you likely already qualify based on your other conditions.
Questions to ask your doctor this week
Based on this week's updates, here are the most actionable questions to bring to your next appointment:
- Diabetes (all patients): "Has my treatment plan been reviewed against the 2026 ADA Standards of Care? Am I on medications that protect my heart and kidneys — not just lower my blood sugar?"
- Diabetes (type 2, not on insulin): "Would a continuous glucose monitor help me manage my blood sugar better, and would my insurance cover it?"
- Diabetes (high cardiovascular risk): "What is my current LDL level? Am I a candidate for a PCSK9 inhibitor like evolocumab (Repatha), in addition to my statin?"
- Cardiovascular (obesity + autoimmune disease): "I have both obesity and [autoimmune condition]. Is a GLP-1 receptor agonist medication appropriate for me, given new data on cardiovascular and mortality outcomes in people with both conditions?"
- Heart attack survivors: "What is my LDL target after my heart attack, and am I reaching it? Are there oral cholesterol-lowering medications I should add?"
- Liver disease (MASLD/fatty liver): "I have been told I have fatty liver disease. Do I also have obesity or type 2 diabetes? If so, am I a candidate for a GLP-1 medication that could help both my liver and my metabolic health?"
- Liver disease (MASLD with elevated liver enzymes): "The June 2026 Hepatology study found betaine at 2–8 g/day reduced liver enzymes in MASLD patients. Is this something worth discussing in my case?"
These updates summarize clinically significant research and guideline developments published June 1–8, 2026. They are a starting point for conversation with your healthcare provider — not a substitute for individual medical advice.
Cover photo: AI-generated illustration for editorial use.
References
- 1Pharmacy Times: ADA 2026 Standards of Care — A Pharmacist's Guide to Cardiorenal Risk Reduction
- 2American Diabetes Association / PR Newswire: 82% of Adults with Type 2 Diabetes Not on Insulin Improve Blood Glucose Levels with CGM
- 3Amgen / PR Newswire: Amgen Presents New Data at ADA 86th Scientific Sessions
- 4Eli Lilly / PR Newswire: Retatrutide Phase 3 TRIUMPH-1 and TRANSCEND-T2D-1 Results
- 5Novo Nordisk / PR Newswire: CagriSema REIMAGINE Program Results
- 6Structure Therapeutics via StockTitan: Aleniglipron Phase 2b ACCESS Results
- 7Managed Healthcare Executive: Berobenatide VESPER IIb Data at ADA 2026
- 8Medscape Medical News: Retatrutide Data Show Dramatic Weight Loss, Other Benefits
- 9AHA Newsroom: GLP-1-based meds linked to fewer heart events in adults with obesity, autoimmune disease
- 10AHA Newsroom: 15 centers selected for groundbreaking research network to transform heart transplant care
- 11Frontiers in Cardiovascular Medicine: HACOL-ACS Trial Protocol
- 12PubMed / GBD 2023 MASLD Collaborators: Global burden of MASLD, 1990–2023
- 13Hepatoma Research: Incretin-based therapies: a new era in metabolic liver disease management
- 14Hepatology: Pilot trials of oral betaine in participants with metabolic dysfunction-associated steatohepatitis
- 15GI & Hepatology News (AGA): MASH label expansion adds few new semaglutide candidates
Add more perspectives or context around this Post.