
Weekly health update: June 1, 2026
This week covers all three disease areas: in diabetes, the FDA approved needle-free inhaled insulin (Afrezza) for children, and a two-year trial showed tirzepatide keeps 60% of early type-2 patients at normal blood sugar. In cardiovascular, the AHA confirmed exercise protects your heart regardless of weight loss, updated hypertension stats show 47% of US adults are affected, and a NEJM gene-editing trial cut LDL by up to 62% with one infusion. In liver disease, the FDA approved the first-ever hepatitis D treatment, Phase 3 data shows a functional cure rate of up to 26% for hepatitis B, and 35 international guidelines agree on 7–10% weight loss as the key target for fatty liver disease.
This past week delivered an unusual cluster of firsts: the FDA approved the only hepatitis D treatment to exist in the US, children with diabetes got their first needle-free mealtime insulin in 100+ years of insulin therapy, a gene-editing trial cut LDL cholesterol by up to 62% with a single infusion, and the American Heart Association (AHA) published a statement telling patients to stop waiting for the scale to move before exercising for their heart. Here's what those four stories mean for you, plus the latest on hepatitis B and fatty liver disease.
Diabetes: a first for kids, and a two-year milestone for tirzepatide
FDA approves needle-free mealtime insulin for children
On May 29, the FDA expanded approval of Afrezza (human insulin inhalation powder, made by MannKind Corporation) to children and adolescents ages 6 and older with type 1 or type 2 diabetes. 1 This is the first needle-free mealtime insulin option available for pediatric patients in more than 100 years of insulin therapy.

A few important safety points your care team will walk through before prescribing:
- Afrezza is not for patients with asthma, COPD (chronic obstructive pulmonary disease), or those who smoke
- A spirometry test (a simple breathing test) is required before starting, and repeated at six months and annually
- Approval is based on the INHALE-1 phase 3 trial of 230 patients ages 4–17; the primary HbA1c endpoint was met in the sensitivity analysis for children who completed inhalation treatment 3
Cost: patients who qualify can access Afrezza for $35 or less per month through MannKind's patient assistance program, MannKind Cares. 1
Question to raise at your next appointment: If your child's mealtime insulin management is difficult — at school, during sports, or because of needle anxiety — ask whether Afrezza is appropriate to try.
Tirzepatide holds 60% of early-type-2 patients at normal blood sugar after two years
A two-year trial result published May 26 in Annals of Internal Medicine found that among adults diagnosed with type 2 diabetes within the previous four years who were not well-controlled on metformin alone, 60.2% of patients taking tirzepatide 15 mg (sold as Mounjaro or Zepbound) reached a normal blood sugar level (HbA1c below 5.7%) — compared with 24.0% in the group receiving standard intensified treatment, which could include other GLP-1 medications. 4
Tirzepatide also produced an additional 8.0 kg of weight loss and 6.2 cm of waist reduction over standard care during those two years. The trial (SURPASS-EARLY, funded by Eli Lilly) was open-label, so patients knew which treatment they received — a design limitation worth noting when interpreting the results.
This is evidence that starting an intensive glucose-lowering approach early in type 2 diabetes may put more patients into remission, though the word "remission" appears cautiously in the research: HbA1c below 5.7% while on medication is not the same as diabetes resolved. What it signals is that the drug class is capable of more than expected.
What to discuss: If you were recently diagnosed with type 2 diabetes and are not meeting your HbA1c goals on metformin, ask your doctor whether tirzepatide or a similar GLP-1/GIP-based medication has a place in your plan.
Cardiovascular: move for your heart, regardless of what the scale says
AHA statement: exercise benefits your heart even without weight loss
On June 1, the AHA published a scientific statement in Circulation confirming what exercise researchers have argued for years: regular physical activity improves blood pressure, insulin sensitivity, cholesterol, and cardiovascular fitness — independently of whether you lose weight. 5 6
Damon L. Swift, Ph.D., FAHA, the statement's lead author and an exercise scientist at the University of Virginia, put it directly: "Physical activity delivers powerful heart and metabolic health gains even when the scale doesn't move."
Why this matters: many patients — and some providers — set exercise aside when weight-loss results stall. This statement from the AHA says that's the wrong response. Forty-two percent of American adults have obesity, and only one in four adults meets current physical activity recommendations. 5 The statement gives your doctor or cardiologist a framework to prescribe exercise as a primary intervention, not a supplement to diet.
Some context on the numbers: exercise alone typically reduces body weight by 3–5% at most. To lose 5% or more through exercise, you'd need 225–420 minutes of moderate-intensity activity per week — well above the standard recommendation of 150 minutes. The AHA isn't downplaying weight management; it's saying don't let the scale be the only measure of progress.
Question to raise: Ask your doctor or cardiologist to assess your current activity level at your next visit, and whether a formal exercise prescription or referral to cardiac rehab is appropriate for you.
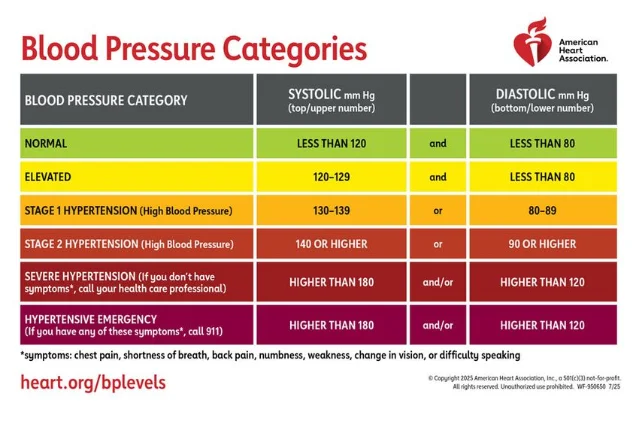
Nearly half of American adults have high blood pressure — and three in four of them aren't controlled
Also on May 28, the AHA released updated statistics alongside a nationwide hypertension awareness campaign: approximately 126 million (47.3%) US adults have high blood pressure, and only about 25.6% have it under control. 7 In 2023, high blood pressure was a contributing factor in 664,470 deaths.
Keith C. Ferdinand, M.D., FAHA, co-vice chair of the 2025 AHA/ACC hypertension guidelines writing committee, framed this clearly: "When you have high blood pressure, it's not just a number on a chart — it's your future at stake; it's your ability to stay present for the people you love."
If you have high blood pressure: Ask your care team at your next visit to review your current medications, home monitoring technique, and whether your target blood pressure goal has changed based on recent guidelines.
Controlling blood pressure, blood sugar, and cholesterol also protects your brain
On May 26, the AHA and American Stroke Association updated a joint scientific statement in Stroke confirming that the same vascular risk factors driving heart disease — high blood pressure, diabetes, high cholesterol, smoking, and physical inactivity — also drive both vascular dementia and Alzheimer's disease. 8 The update, which replaces the 2011 version, recognizes that most age-related cognitive decline is a mixed process involving both vascular damage and neurodegeneration at the same time.
In plain terms: the habits and treatments protecting your heart also protect your brain. Every conversation you have with your doctor about blood pressure, A1c, and cholesterol management is doing double duty.
A glimpse of what may come: gene editing and LDL cholesterol
Published May 25 in the New England Journal of Medicine, the first phase 1b trial of VERVE-102 — an in-body base-editing therapy that permanently inactivates the PCSK9 gene in the liver — lowered LDL (low-density lipoprotein) cholesterol by up to 62% with a single IV infusion in 35 patients with familial hypercholesterolemia or early coronary artery disease. 9 The effect held for at least 12 months in participants followed that long.
To be clear on where this stands: this was a 35-patient phase 1b safety and dose-finding study. VERVE-102 is not approved or available for clinical use. No dose-limiting toxicity appeared, and mild-to-moderate infusion reactions resolved. The trial is run by Verve Therapeutics, a wholly owned subsidiary of Eli Lilly.
What makes it noteworthy is the mechanism. PCSK9 is the protein that regulates how much LDL the liver clears from the blood. People born without a functional PCSK9 gene have lifelong low LDL and far fewer heart attacks. This therapy is attempting to replicate that genetic state — permanently — in a single infusion. It is early, but the biology is well-validated.
Liver: two historic firsts for hepatitis
FDA approves the first-ever treatment for hepatitis D
On May 22, the FDA granted accelerated approval to Hepcludex (bulevirtide-gmod, made by Gilead Sciences) for adults with chronic hepatitis delta virus (HDV) infection who do not have cirrhosis or have compensated cirrhosis. 10 This is the first and only FDA-approved treatment for HDV in US history.
HDV is a satellite virus — it can only infect people who already have chronic hepatitis B (HBV), because it depends on HBV proteins to replicate. The combination is more severe than HBV alone: patients progress to cirrhosis faster and face a five-year mortality rate of up to 50% in those who reach that stage. An estimated 40,000–80,000 people in the US carry both. 11
Hepcludex is given as a daily subcutaneous injection (similar to the self-injections used in diabetes care). In the phase 3 MYR301 trial, 48% of patients on Hepcludex had a combined response at week 48 (undetectable HDV RNA or a significant drop, plus normalized liver enzyme levels) compared with 2% in the delayed-treatment group. 10
Important safety note: The FDA label includes a boxed warning — stopping Hepcludex without guidance can trigger a severe flare of both HDV and HBV. Any patient on this medication should not discontinue without close medical supervision; liver function must be monitored for at least six months after stopping.
Wendy Carter, D.O., acting director of the FDA's Office of Infectious Diseases, noted that the approval "fills a critical gap in care for patients with chronic HDV infection, who until now have had no FDA-approved therapies available."
If you or a family member has chronic hepatitis B: Ask your hepatologist or gastroenterologist whether you have also been tested for HDV co-infection. The two viruses require different management, and HDV testing is not always part of routine hepatitis B monitoring.
Hepatitis B: phase 3 data shows functional cure in nearly 1 in 5 patients
On May 28, GSK reported results from two phase 3 trials (B-Well 1 and B-Well 2) of bepirovirsen, an investigational antisense oligonucleotide (a drug designed to block a specific protein's production), published in the New England Journal of Medicine. 12
The results across both trials combined:
| Patient group | Functional cure rate (bepirovirsen) | Functional cure rate (placebo) |
|---|---|---|
| All patients in the trial (HBsAg ≤3,000 IU/mL at baseline) | 19% (233 of 1,220) | 0% (0 of 614) |
| Lower viral activity subgroup (HBsAg ≤1,000 IU/mL at baseline) | 26% (200 of 768) | 0% (0 of 393) |
"Functional cure" is defined as no detectable hepatitis B surface antigen (HBsAg) and no detectable HBV DNA in the blood for at least 24 weeks after stopping all treatment. Current standard treatments — nucleoside analogs (NAs) like tenofovir and entecavir — achieve functional cure in only 1–3% of patients. Those drugs suppress the virus but rarely eliminate it. 12
The lower viral activity subgroup (HBsAg ≤1,000 IU/mL) represents approximately 45% of all people diagnosed with chronic hepatitis B globally. HBsAg clearance is associated with an 89% reduction in liver cancer risk and a 62% reduction in overall mortality in the literature.
Bepirovirsen is not yet approved anywhere. The FDA has it under priority review (with Breakthrough Therapy designation), and a first regulatory decision is expected in Q3 2026. GSK has also filed with the European Medicines Agency (EMA), in Japan, and in China.
What this means if you have chronic hepatitis B: Your current treatment is not changing today — but if you've been managing HBV on long-term antivirals, this is a milestone worth discussing at your next hepatology visit. The standard of care may look different within the next year.
MASLD lifestyle management: what 35 international guidelines agree on
A review published in Hepatology in May synthesized 35 international guidelines on metabolic-associated steatotic liver disease (MASLD, also called NAFLD in older literature) and found strong agreement on the lifestyle core: lose 7–10% of body weight to improve liver inflammation and fibrosis, and aim for 150–300 minutes of moderate-intensity or 75–150 minutes of vigorous physical activity each week. 13 Reducing commercial fructose intake (found in many processed foods and sweetened drinks) was also widely recommended.
Where the 35 guidelines are thinner: mental health support, social determinants of health, and digital health tools are mentioned in fewer than a quarter of them, despite being relevant to whether lifestyle changes actually stick.
If you have been diagnosed with fatty liver disease: The goal is 7–10% weight loss — not a crash diet. A 5–10 lb reduction in someone weighing 150 lbs can meaningfully reduce liver fat. Ask your gastroenterologist or primary care provider what a realistic target looks like for you.
These updates summarize clinically significant news published May 25 – June 1, 2026. They are a starting point for conversation with your healthcare provider — not a substitute for individual medical advice.
Cover image: Afrezza inhaler. Image courtesy of MannKind Corporation
References
- 1MannKind: FDA Approves Afrezza for Children Ages 6+
- 2AJMC: FDA Approves Inhaled Insulin for Children, Adolescents With Diabetes
- 3MannKind Afrezza News
- 4Del Prato S, et al. SURPASS-EARLY — PubMed
- 5AHA Newsroom: Move more for your health, not just for the scale
- 6AHA Professional: Role of Physical Activity in Obesity Treatment and Cardiometabolic Health
- 7AHA Newsroom: The lowdown on high blood pressure
- 8AHA Professional: Vascular Contributions to Cognitive Impairment and Brain Health
- 9NEJM: In Vivo Base Editing of PCSK9 with VERVE-102 (PubMed)
- 10FDA: FDA Approves First Treatment for Chronic Hepatitis Delta Virus (HDV) Infection
- 11Gilead Sciences: FDA Grants Accelerated Approval to Hepcludex
- 12GSK: Bepirovirsen achieves unprecedented functional cure rates
- 13Hepatology: Narrative Review of Lifestyle Management Guidelines for MASLD
Add more perspectives or context around this Post.